BREAKING THE CYCLE: Alcoholism and Fetal Alcohol Syndrome In Native American Indians
N.R. Fox © 2004
(This report was originally written in 2004 as a research paper. Although several years have passed, the incidence of alcoholism in Native America continues to rise and with it, crime, rape, and poverty are also on the rise. It is the author's belief that the information within this report remains just as important and valid as when it was written.)
When one contemplates the concept of Fetal Alcohol Syndrome (FAS) based on current and cultural data, the facts have not always been available to the general public. Unfortunately stereotyping and myths tend to make up the mass of what many believe to be factual details of this debilitating and preventable disease. Fetal Alcohol Effects (FAE) is a similar but less profound condition which has fewer symptoms than FAS and will not be discussed in this report.
Before alcoholism can be understood, it must first be defined. Dr. David Ohlm defines alcoholism as a "chronic, progressive, incurable disease, characterized by loss of control over alcohol and other sedative drugs."
“In an alcoholic, when the body is digesting the alcohol, it produces an excess of the neurotransmitters tetrahydroisoquinolines, or TIQs. These TIQs are addictive, and create opiate substances, or an endorphins, which is a stimulant. These TIQs behave similar to cocaine, in their addictiveness, and affects on the brain (Ohlm). In social drinkers, the reaction does not take place and do not create these TIQs, but depress the production of endorphins, therefore feeling bad, having the alcohol act as a depressant. Some people do create these TIQs, and feel good, causing the alcohol to act as a stimulant, which can be addictive and cause alcoholism. To demonstrate the effects of TIQs, rats have been used. There is a strain of genetically engineered rats which detest any alcohol. They would die of thirst before even drinking 3% alcohol. But, when injected with TIQs, the rats prefer drinking 100 proof alcohol over water. This demonstrates the addictiveness, and how the TIQs override other inhibitions. All of these physiological differences provide for increased chances for the occurrence of alcoholism, and all of them could very likely be passed through genetics” (Esser).
In 1987 most reported cases of FAS in the United States came from study sites where the mothers were black or Native American and of low socioeconomic status. According to the CDC catchment study in 1989, incidences of FAS per 10,000 births were Asians 0.3, Hispanics 0.8, Whites 0.9, Blacks 6.0, and Native Americans 29.9 (Narconon). Other studies have shown that Native Americans are 33% more likely to have a child with FAS than those of other races (Stump), while the US Department of Health and Human services report that FAS among Native Americans children can be as high as 103 in every 10,000 births (Kellerman).
So the question arises, why is there such a high incidence ratio for Native Americans? There is, at present, much controversy in the medical community regarding the possible underlying cause(s) for FAS in any culture. However, Native Americans also have a higher ratio per capita for both those raised within the culture, as well as those not raised within the culture (Streissguth, et al). Studies are showing that the age-old debate between nature vs. nurture,bears further research into this medical and ethnic phenomenon (Prescott).
While there is no intent to discredit or exclude the rising number of FAS births in other races and cultures, historically FAS has been predominantly unrecognized in Native American families. But to establish a historical precedent there must be an understanding of the diagnostic tests that are used to determine FAS and the realization that until recently, Native children were less likely to be tested or treated unless raised within a non-native family. Due to the physical features of Native infants, facial recognition is the least accurate measure of diagnosis; thus the expensive and time-consuming procedures that follow were not utilized for a people whom the government coerced into sterilization procedures in the early 1970’s. From the government’s prospective, it was easier to intentionally abort hundreds of pregnancies or sterilize over 12,000 Native women, most without their consent or full knowledge of the procedure, than educate them on the dangers of drinking while pregnant (England).
As is obvious in the following diagram, the physical characteristics of FAS closely resemble those of a normally developed Native American child. The squat nose, epicanthal eye folds, thin upper lip, and flat midface make it increasingly difficult to diagnose a Native child with FAS unless the maternal drinking habits of the mother are known in advance. Many of these features become less pronounced at the children grow older. Children with FAS are more likely to have congenital heart disease, poor coordination, abnormally formed organs and mental retardation (Leung).
A diagram of the different facial dysmorphologies a child with FAS may display
In infants FAS is much easier to diagnose than it is in adolescents and adults. FAS can be diagnosed when patients have a positive history of maternal alcohol abuse during pregnancy and growth deficiency of prenatal origin (height and/or weight); a pattern of specific minor anomalies that include characteristics generally defined by a small head, lack of vertical ridges between the nose and lip, thin upper lip, narrow eye slits, delayed adjustment, attention deficits, learning disabilities, low IQ, and seizures. While mental retardation does not always accompany FAS, most patients have major psychosocial problems and adult victims may have difficulty maintaining successful independence. Other patients, however, may show no physical signs of FAS and diagnosis is not made until much later in life, thus leaving the patient feeling as if he or she were simply a “bad seed.”
Steph Braddock, director of the Missouri Fetal Alcohol Syndrome Center in Columbia, says the ideal time to diagnose FAS is between the ages of eight months and eight years. “Diagnosis will entail proper screenings and testings to pinpoint the patient’s strengths and weaknesses and ensure the child has a proper intervention plan. We also want to make sure the mothers are in treatment. We can’t undo what has happened, but with appropriate intervention, we can provide treatment and, we hope, prevent it from happening again in the future.” Braddock also says that health care providers may not initially diagnose children with FAS, although many of the neurobehavioral problems exhibited, such as poor communication or memory, may lead to secondary disabilities and behavior problems. Although the ideal age is commonly overlooked in these diagnostic procedures, Braddock says that children will benefit from screening even if they are older than eight years old (Ghan).
The difficulty with diagnosing adolescents and adults arises as the abnormal physical characteristics eventually give way to normal physiological growth. The physical and mental manifestations of the syndrome in adolescents and adults have remained an important unsolved area of investigation (Steissguth, et al).
(Photo Courtesy of Teresa Kellerman)
How, then, do genetics come into play regarding the higher rate of Native Americans with FAS? Scientists have known for some time the rate of alcohol metabolism can vary as much as threefold among people with similar drinking habits and recent studies indicate that the development of alcoholism is influenced by both genetic and environmental factors. "It appears that the development of alcoholism is not a case of genetics versus the environment; it is one of genetics and the environment," says Dr. Ting-Kai Li, distinguished professor of medicine and biochemistry at the Indiana University School of Medicine in Indianapolis. Dr. Li’s research has identified two specific genes that protect against heavy drinking. These genes are particularly prevalent among Asians. This research has also shown that Native Americans do not have these protective genes. The transformation that is particularly effective is a mutation of the gene for the enzyme aldehyde dehydrogenase (ALDH), which plays a major role in metabolizing alcohol. Medical research has shown that alcohol is metabolized principally in the liver, where it is converted first to acetaldehyde by the enzyme alcohol dehydrogenase (ADH). Alcetaldehyde is then converted to acetate by the enzyme aldehyde dehydrogenase (Kibbey).
A genetic study by Denis Lowe Viljoen, head of the department of human genetics at the South African National Health Laboratory Science and University of the Witwatersrand faculty of Health Sciences, has shown the incidence of FAS cases in Native American children to be eight per one thousand, while the rate for the White population was 0.33-2.2 and 2.29 for inner city African Americans. Amanda Krause, a researcher and associate professor with Mr. Viljoen, states, “There is good scientific evidence that FAS, like virtually all diseases, has some genetic and some environmental influences.” She points out that ADH is one of two enzymes that act sequentially to metabolize alcohol in the liver and it is ADH that converts alcohol to acetaldehyde (Kibbey).
What these studies have shown is that acetaldehyde produces unpleasant physiological reactions even at low concentration, so the presence or absence of the gene mutation affecting aldehyde dehydrogenase in turn affects drinking behaviors. When acetaldehyde is not rapidly converted to acetate, the results are dramatic: a rapid increase in blood flow to the skin of the face, neck, and chest, rapid heartbeat, headache, nausea, and extreme drowsiness occur. As would be expected, this aversive reaction affects drinking behavior (Streissguth, et al).
A number of researchers have demonstrated that EEG patterns are different in alcoholics and non-alcoholics. It has been determined that the differences are not that of alcohol use, but that these differences are present at birth in identical twins. Individuals at risk for alcoholism can be differentiated on the basis of their EEG alpha activity. Alcoholics have greater increases in slow alpha activity and greater decreases of fast alpha activity after use of alcohol; thus a reduced P300 wave is a good predictor of alcoholism.
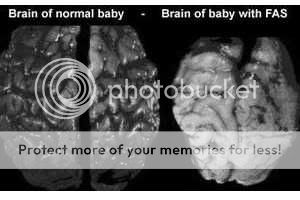
The following graphic shows the biological deviations that can occur in the brain due to alcohol consumption during pregnancy. As noted, the corpus callosum in the brain of a normal child shows normal regular growth; while the brain of the child suffering from FAS shows a complete absence of the corpus callosum. Responsible for maintaining much of the communication between regions in different hemispheres of the brain, the absence of the corpus callosum, known as agenesis of the corpus callosum (ACC) can result in mental retardation, cerebral anomalies, eye anomalies, and epilepsy. Autopsies of infants diagnosed with FAS have shown evidence that maternal consumption of alcohol during pregnancy directly affects the development of embryonic brain tissue and can easily result in ACC (Indiana University).
Consider the child who portrays no outward physical symptoms of FAS yet shows a substantial retardation in intellectual, social, emotional, and spiritual growth. Typically, the child would be diagnosed with one of many behavioral disorders (most commonly Attention Deficit Hyperactivity Disorder) and medicated while the underlying effects of FAS remain unrecognized, undiagnosed, and summarily untreated.
(Photo courtesy of Christensen)
Recent studies have shown that alcoholism relapse can be predicted by brain waves. Alcoholics are said to use alcohol, sugar, nicotine, and caffeine in vain attempts to quiet their irritable brain waves (Dapice, et al). It is easy to attribute the issue of genetics coupled with environment and the growing number of Native American children with FAS. With the number of alcoholic persons of European ancestry rising, it is not difficult to perceive the number of culturally separated or mixed blood Native American children stricken with FAS rising as well.
Statistical data confirms an alarming increase in Native American alcohol addicts. Mail and Johnson concluded in a 1993 study that "alcohol is the drug of choice among American Indian people," however, the tragic trend over the years shows recent signs of improvement that bear closer scrutiny.
For those over the age of 12 in 2000, the percentage of "current drinkers" (those who drank in the past month) among the 4 million American Indians and Alaska Natives (35 percent) is much lower than both Whites (51 percent) and Hispanics (40 percent), and only slightly higher than Blacks (34 percent). However, 19 percent of American Indian youth 12 to 17 are past month drinkers—the highest of the major ethnic groups (though the White figure is close—18 percent). For persons over 26, the Native American past month rate is actually the lowest of all. The alcohol abuse problem among American Indians/Alaska Natives appears to be concentrated in the young and the so-called “heavy drinkers” over 26. Binge drinking rates (drinking five or more drinks on one occasion at least once a month) for youth 12 to 17 are highest for Native Americans (12.8 percent do it, versus 11.9 percent for Whites and 11 percent for Blacks). For Native youth who practice "heavy alcohol use" (defined as binge drinking five times a month or more), the rate 1999 to 2000 has declined significantly, from 4.6 percent to 2.9 percent (rates were at least twice as high a decade ago). But after 26, the 7.4 percent rate of heavy alcohol users is highest among Native Americans, and is increasing, while most other groups’ severe use rates are stable or declining (SAMHSA).
And what of nature vs. nurture? A study involving a 37-year-old mixed blood Native American female shows that nurture can play the same role in the development of alcohol abuse as nature.
Born addicted to alcohol and other drugs, the subject was given up for adoption at birth and placed within a non-native home with no history of alcohol or drug use. By the age of five, she had taken her first drink of alcohol, stating it was a “familiar and welcomed experience.” Although she had not been subjected to alcohol in the home, she now believes that she was an alcoholic at birth, but a willing alcoholic by the age of sixteen (Fox). Abuse was also an issue in the home and research has shown that abusive situations can contribute to the desire for alcohol and other drugs (Dapice, et al). Subsequently, the subject has a biological family history of substance abuse for at least 13 generations.
Medical tests as an adult for unexplained pain and muscle tremors revealed encephalic characteristics for FAS and childhood photographs portrayed the noted physical characteristics. Developmental delays, seizures, and a diagnosis of Attention Deficit Hyperactivity Disorder as well as other psychosocial and mental diagnoses were concurrent with the systemic disorders associated with FAS (Streissguth, et al) (Dapice, et al).
Typical psychological symptoms of FAS can include immature social development, being overly friendly to strangers, lack of sexual boundaries, emotional liability, poorly developed conscience, lack of consistent impulse control, good expressive language skills, talented in art, music, or mechanics, attention deficit; not always hyperactive, but easily distracted by external stimuli, short-term memory deficits, inappropriate social interactions, difficulty managing money, a poor concept of time, grandiose ideas and unrealistic life goals, distorted perceptions, poor judgment, vulnerability and naiveté (Kellerman).
Children afflicted with FAS are unfortunately at risk for even further psychological and/or psychosocial difficulties as they mature. Learning processes are interrupted or distorted, making the typical educational system inadequate to successfully instruct and prepare the child for independent adulthood. In areas such as reservations or inner cities where the majority of Native American children afflicted with FAS are raised, it becomes painfully obvious that limited opportunities, coupled with distinct learning disabilities sentence the child to a life of poverty and an exceedingly high risk of further substance use/abuse as an adult.
The level of distractibility experienced increases with the difficulty of the task at hand. A link has also been established between FAS and Attention Deficit Disorder (ADD). 85% of children with FAS also have ADD. In these particular children, the onset is usually earlier, and encompasses more severe developmental, psychiatric, and medical aspects.
Impulsive behavior is another commonly noted characteristic of children with FAS. These symptoms can manifest by having the children place themselves in dangerous situations where they can find themselves retaliating in anger by verbally or physically means to difficult situations. This aspect of behavior often diminishes during adolescence.
Memory skills in children with FAS may be affected at three different stages (depending on the length of time the fetus was exposed to alcohol, the degree, and during which trimester(s). If the sensory abilities were compromised in development, it would affect the children’ ability to take in’” memories. If the storage abilities were compromised during development, than memories will not be sorted as effectively. If the retrieval systems were compromised during development; than the child will not always be able to retrieve memories that they have retained.
Finally, FAS children have a particularly hard time remembering sequences of information (Leung).
On a social level, children with FAS are at a distinct disadvantage and often find themselves ostracized by their peers. FAS children have fewer inner resources for coping with normal stresses and pressures of everyday living. FAS children also experience more problems in adapting to change and making choices.
Some children with FAS excel in the area of motor skills; these are good activities to build self-esteem and lifelong leisure pursuits for children suffering from FAS. Others children that suffer from the disorder have significant problems with gross & fine motor skills. Learning coordinated movements (such as writing) may be more delayed in FAS children.
FAS children experience significant problems in communicating due to the face that they develop their language skills at a slower rate. Often FAS children are observed to use “cocktail party conversation,” fluent words which are void of content.
Ironically, children with FAS are often eager to learn. This is a resource that must be encouraged and refined from the beginning in order to be maintained.
Amazingly enough, children who suffer from FAS are often creative, musical, and artistically gifted. Furthermore, artistic activities can greatly expand the range of thoughts, images, and feelings in all children but it is especially helpful for children with FAS. For instance, music can help the child to perceive, explore, communicate, and reflect upon these things without have to use written form. These subject areas provide FAS children with other “languages of communication” which they often find easier to use.
Many FAS children have trouble learning science skills and processes. This stems from problem solving deficiencies (deduction and inference). Also, they may lack the development of fine motor skills that are necessary to manipulate microscopes. Another common issue with children suffering fro FAS is the inability to understand instructions, or describe observations.
Sequential computation and problem solving also seem to be more difficult for FAS children. Problems with abstract and complex ideas also make math particularly hard for these children.
Underlying language disabilities can also cause difficulties in this area for children with FAS. Sound-symbol associations do not come as easily as to their peers. By intermediate grades, a plateau in reading and writing progression is often reached. This could include the inability to progress in reading and writing skills causes the expectations of teachers unattainable for these children. A slowness to develop abstract thinking is another factor that can make reading comprehension hard for these children. Organizing thoughts in a sequential manner is necessary in writing - another difficult area (Leunng).
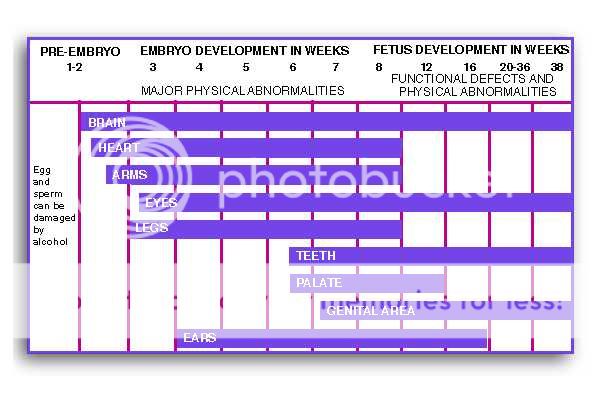
Stages of the Developing Fetus
Guidelines of Care for children with Special Health Care Needs
Fetal Alcohol Syndrome and Fetal Alcohol Effects
 (Minnesota Department of Health 1999)
(Minnesota Department of Health 1999)
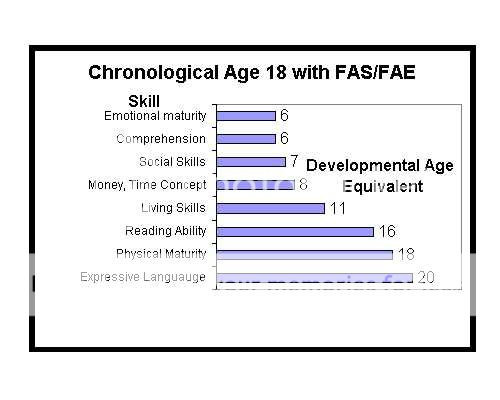
The graphs below show the progression of disabilities and life-long complications faced by victims of FAS. Note the greatest factor of challenge is that of mental health (first graph) combined with a low level of emotional maturity (second graph) which creates the issues lack of boundaries and consequential thinking.
(Adapted from Streissguth, p.108, 1997)
(Adapted from AFM, Undated)
Fetal alcohol syndrome occurs among Alaska Native newborns at twice the national average, and 73 percent of the women who give birth to these FAS children report being sexually abused as a child. Still, Native American resilience has been as legendary as it’s near genocidal history. With a heightened awareness of cultural traditions, prevention specialists have learned some lessons: use American Indians as staff in mental health/substance abuse clinics whenever possible; incorporate cultural concepts and bi-cultural realities within programs; target prevention at early ages (SAMHSA).
While the only prevention for FAS is to abstain from alcohol, it has become apparent that the application of the prevention is not so simple. There is no borderline too much or too little; one drink is too much during pregnancy and the repercussions are immeasurable and undeniably avoidable.
Addiction is not a cultural pastime for Native Americans, but rather an ignored continuing means of attempted genocide (Dapice, et al). Lack of education, treatment options, and appropriate counseling for the Native Americans in understanding the cause and consequences of FAS has been the major contributing factor to the ongoing challenge of eradicating this destructive and needless disease that should have never been introduced.
Works Cited
Christensen, Damaris. Article: Science News. Washington: Jul 8, 2000. Vol. 158, Iss. 2; p. 28 (2 pages) “Sobering work: Unraveling Alcohol's Effects on the Developing Brain” Online. Proquest. Accessed February 28, 2005.
Dapice, Ann N., PhD; Inkanish, Clark, ICADC; Martin, Barbara, B.S.; Brauchi, Pam, MHR, LPC. Article: Native American Times. From The Oklahoma Indian Times, Inc. “Killing Us Slowly: When We Can’t Fight, and We Can’t Run.” Online.
. Accessed May 9, 2003.
England, Charles R. “A Look at the Indian Health Service Policy of Sterilization.” Online. < http://www.dickshovel.com/IHSSterPol.html >. Accessed March 02, 2005.
Esser, James. “Genetic Influences on Alcholism.” 15 May 1997. Available online at < http://www.brainerd.net/~esserste/essays/alcohol.htm >. Accessed17 March 2005.
Fox, I.G. “Because I Can.” Autobiography. Unpublished. Excerpt. Chapter 6. 2003.
Ghan, Cheri Article: @mizzou. News From Missouri’s Great State University. “MU Houses First Fetal Alcohol Clinic.” Online. < atmizzou.missouri.edu/ jun04/FetalAlcohol.htm >. Accessed February 28, 2005.
Indiana University. “Agenesis of the Corpus Callosum, The Literature 01.” Online. No author cited. and . Accessed March 23, 2005.
Kellerman, Teresa. Photo Credit. “FAS and the Brain.” Online. < http://www.come-over.to/FAS/FASbrain.htm >, < http://www.come-over.to/FAS/NAFAS.htm >, and < www.come-over.to/ FAS/brochures/ >. Accessed Febrauary 28, 2005.
Kibbey, Hal. University of Indiana. “Genetic Influences on Alcohol Drinking and Alcoholism.” Online. . Accessed February 28, 2005.
Leung, Grace. “Research Project: Fetal Alcohol Syndrome & Fetal Alcohol Effects.” Online. . Accessed March 23, 2005.
Narconon. “Fetal Alcohol Syndrome.” Narconon of Oklahoma. Article. Online. < http://www.stopaddiction.com/narconon_alcohol_fetal.html>. Accessed February 28, 2005.
Prescott, Carol A. Virginia Institute for Psychiatric and Behavioral Genetics. “Nature vs. Nurture in Progression to Alcoholism.” The Brown University Digest of Addiction Theory and Application. October 1999 v18 i10 p5. Article. Online. Infotrac: Health Reference Center – Academic. Accessed February 28, 2005.
Streissguth, Ann Pytkowicz; Aase, Jon M.; Clarren, Sterling K.; Randels, Sandra P.; LaDue, Robin A.; and Smith, David L. “Fetal Alcohol Syndrome in Adolescents and Adults.” The Journal of American Medical Association, April 17, 1991 v265 n15 p1961. Article. Online. Infotrac: Health Reference Center – Academic. Article A10666511. Accessed February 28, 2005.
Stump, Dan. “Fetal Alcohol Syndrome and Other Drug-Related Birth Defects.” Online. < http://www.msu.edu/~stumpdan/hs/fas.htm >. Accessed Febrauary 28, 2005.
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Substance Abuse Prevention (SAMHSA). Prevention Alert. “American Indians/Alaska Natives and Substance Abuse.” Volume 5, Number 16 November 22, 2002. Accessed 17 March 2005. < http://ncadi.samhsa.gov/govpubs/prevalert/v5/10.aspx >.